Introduction
For many years, there has been great debate on how we differentially diagnose between a pressure ulcer and a diabetic foot ulcer.
This can be relevant in knowing: –
- What screening assessment tool to use
- Treatment pathways to follow
- The duty of care to assign responsibility
Let’s Deep Dive into the Depth of the issue:
Firstly, we remind ourselves what normal looks like. Skin is formed of 2 main layers: the dermis and the epidermis.
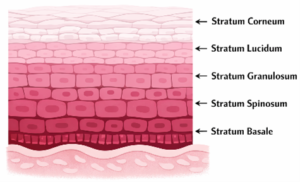
Epidermis: –
Is comprised of 4 layers (5 on the palms of the hands and soles of the feet), these layers are the stratum basale, stratum spinosum, stratum granulosum, stratum lucidum and the stratum corneum. These layers act like a first-line barrier to the world around us.
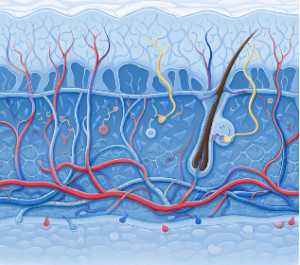
Dermis: –
This layer is what contains our nerve endings, capillary loops, hair follicles, sweat glands and arterioles and venules.
Ulcerations can be caused by ischemia (impaired blood flow), pressure, injury, malignant (fungating wounds), inflammation, Fluid retention and metabolic issues. Knowing the root cause of these ulcers can help us speed up healing and restore a quality of life to our patients that they may not enjoy if these issues persist.
What is a Pressure Ulcer
Aetiology
Pressure ulcers are caused by pressure, or pressure in combination with shear forces [EPUAP/NPIAP/PPPIA, 2019; Gefen, 2020; BMJ, Best Practice 2021; OHID, 2022; Causes | Background information | Pressure ulcers | CKS | NICE].
Pressure ulcers can occur due to the forces of a person’s body weight or as a result of externally exerted forces, such as those applied by a medical device and/or other objects [EPUAP/NPIAP/PPPIA, 2019; Gefen, 2020;Causes | Background information | Pressure ulcers | CKS | NICE].
Assessment
There are a number of assessment tools you can use for a patient to assess to see if it is a Pressure Ulcer and what category it is.

Treatment
Key Pressure Offloading Solutions
Pressure offloading is a cornerstone of effective wound prevention and management of pressure ulcers. While no list is completely exhaustive, the most commonly used approaches include:
Foot-Based Offloading – (Heel Ulcer)
Specialist footwear- designed to redistribute plantar pressure
Orthotic supports – that correct biomechanical loading
Total Contact Casting – the gold standard for offloading diabetic foot ulcers
Bed-Based Pressure Redistribution
Pressure redistribution mattresses and overlays
Lateral turning systems – that automatically reposition patients
Pressure offloading boots – to protect the heel and ankle
Seating and Mobility Support
Pressure redistribution cushions and specialist seating systems
Support Surface Technologies
Modern pressure – relieving systems typically use one of the following technologies:
Low-friction air cell systems
Static surfaces – constant pressure redistribution
Dynamic surfaces – alternating pressure to relieve tissue load
Hybrid systems – combining static and dynamic features
Together, these technologies aim to reduce sustained tissue pressure, improve perfusion, and protect vulnerable areas from breakdown.
Plan
Effective management of pressure ulcers requires a structured approach that addresses vascular status, wound care, and pressure offloading.
Assess Blood Flow in the Extremity
For pressure ulcers occurring on the lower limb or foot, vascular assessment is essential. The clinician must determine whether the ulcer has developed due to:
- Transient ischaemia caused by sustained pressure
- Underlying arterial insufficiency
This distinction is critical because poor arterial supply significantly affects healing potential.
Objective vascular assessment should be performed using quantifiable and reliable measurements, such as Doppler waveform analysis and pressure indices (as provided by BlueDop). These measurements allow clinicians to:
- Identify adequate perfusion for healing
- Detect peripheral arterial disease
- Stratify patients into moderate-risk monitoring or high-risk referral pathways
Patients with significant arterial compromise should be referred promptly for vascular specialist assessment.
Establish an Appropriate Wound Care Plan
Once vascular status is understood, treatment of the ulcer can be tailored to the wound characteristics.
The level of exudate typically determines dressing frequency:
- Low to moderate exudate: dressing changes once weekly
- Moderate to high exudate: dressing changes up to twice weekly
Each treatment episode should include:
- Thorough cleansing of the wound
- Debridement where appropriate to remove non-viable tissue
- Application of a suitable dressing to manage moisture balance
- Detailed documentation of the wound
Implement Effective Pressure Offloading
Without effective pressure relief, even well-managed wounds will struggle to heal.
Pressure offloading strategies may include:
- Specialist footwear or orthotic supports
- Pressure redistribution mattresses or overlays
- Offloading boots or cushions
- Lateral turning systems for immobile patients
Consistent adherence to offloading strategies is essential to reduce tissue loading and allow healing to occur.